Why We Updated Suicide Risk Reporting in MindMetrix

May 19, 2026 | Jillian Fortain, Ph.D., LP
This is the first piece I've written for Metrix on the Mind, and I wish it were about almost anything else. But it felt important enough that I didn't want to wait for a happier occasion.
Recently, I lost a long-time client to suicide.
I share that carefully, and with deep respect for her privacy. She was many things to many people: always thoughtful, kind, witty, loyal, dependable, and hard-working. She struggled with suicidal thoughts and behaviors for many years. She was engaged in care, participated actively in treatment, and followed the recommendations of her treatment team. I have so much compassion for the parts of her that just wanted the pain to stop, to be done fighting and struggling - and I am so incredibly sad that she’s gone.
Her death has been a devastating reminder of something we as clinicians know but never stop wrestling with: Even with careful assessment, strong treatment engagement, safety planning, and coordinated care, suicide risk can remain difficult to detect, impossible to predict with certainty, and never really in our control. Suicidal crisis can escalate quickly, and our clients have free will.
But we can keep asking the question, “How do we improve detection, and how do we better support the people in front of us?” That question shaped several recent updates to MindMetrix.
MindMetrix has always included suicide risk screening with the Columbia-Suicide Severity Rating Scale (C-SSRS), specifically the Screener, Recent version. The C-SSRS is a strong, well-validated tool for flagging people at elevated risk who warrant further assessment for suicidal thoughts and behaviors.
But a screener is only ever a screener. It can't capture every facet of something as complex as suicide risk. It organizes information consistently and flags acute risk, but it can't predict suicide, remove uncertainty, or get past every barrier to disclosure.
Disclosure is one of the hardest parts of assessment, because people have real, valid reasons to hold back. They may fear hospitalization, judgment, losing their autonomy, or burdening the people they love. Some minimize how bad things are. Some carry deep shame about their thoughts or history. Some don't see themselves in the language we use. It takes courage and trust to be that vulnerable with us.
That's part of why structured screening is important. A well-designed question can open a quieter door, a way for someone to say yes to something they aren't ready to say out loud yet.
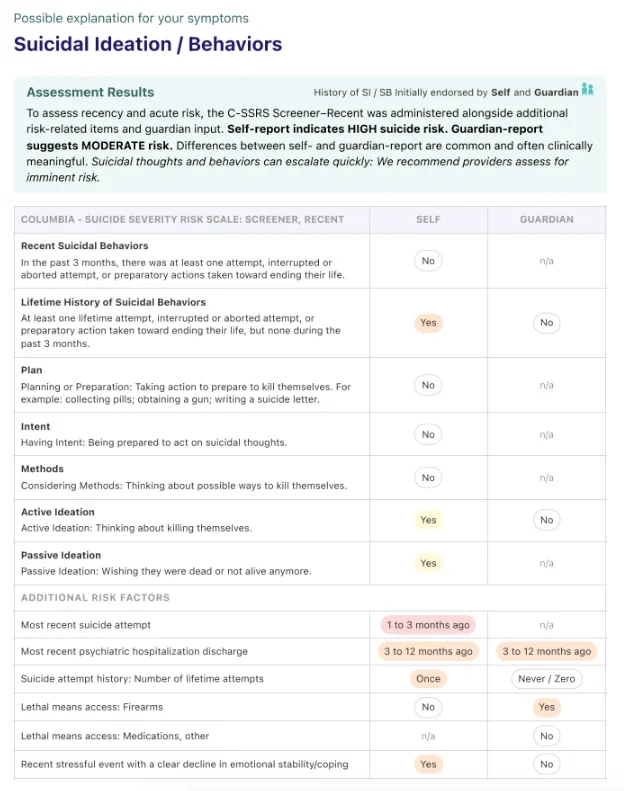
As part of our work to support clinicians, we’ve improved how suicide-related information shows up in MindMetrix reports. In addition to the C-SSRS, we added new content that taps into some of the strongest predictors of future suicidal behavior. Responses on these new items can elevate the client’s overall suicide risk level, above what was identified on the C-SSRS alone.
These include additional risk factors include:
- Recent suicide attempt,
- Recent discharge from psychiatric hospitalization, and
- Number of prior attempts
We also added more visibility around contextual risk factors that can be clinically meaningful - and may need to be investigated further - when suicidal thoughts or behaviors are present.
These contextual risk include:
- Access to lethal means
- Recent destabilizing events
- Differences between self-report and guardian-report, for teens
- Guardian uncertainty, for teens
No single item can predict suicide with certainty. But the right information, displayed clearly, can help clinicians see what needs closer attention, follow up more effectively, involve other supports as needed, such as family/parents, safety planning, lethal means counseling, or a higher level of care. The updated section and new content are there to support our clinical judgment, not stand in for it.
I won't pretend that improving our tool makes a loss like this easier. It doesn't. But it gave me somewhere to put it. If a clearer report and the additional risk-related items help another clinician detect risk sooner, focus their follow-up assessment more effectively, or better support their client in taking one more step toward safety while there is still time, then her death will have done something for someone she never met. And I think she would have really liked that.
If you or someone you know may be in immediate danger, call 911 or go to the nearest emergency department. In the U.S., call or text 988 to reach the Suicide & Crisis Lifeline.
Ready to boost your practice?
Try 3 complimentary assessments on us.