Evaluating the Impact of MindMetrix on Psychiatric Symptoms Over Time
Presented at NEI Spring 2026
Authors: Joel L. Young, R. N. Powell, Anna Powell, Lisa L. M. Welling, Lauren Granata, Jaime Saal, Margot Nash
Affiliations: Rochester Center for Behavioral Medicine; MedaData, LLC; School of Medicine, Wayne State University; Department of Psychology, Oakland University; MindMetrix, LLC
At the NEI Spring Congress, May 1–3, 2026, researchers from Rochester Center for Behavioral Medicine, MedaData, Wayne State University, Oakland University, and MindMetrix presented findings from a retrospective longitudinal study examining whether including MindMetrix as part of psychiatric intake is associated with changes in depression, anxiety, ADHD symptoms, and overall psychiatric symptom burden over time.
Aim
This study aimed to determine whether including the comprehensive mental health assessment, MindMetrix, upon intake to psychiatric treatment is associated with trajectories of depression, anxiety, and ADHD symptom severity.
Why This Study Matters
Psychiatric disorders frequently co-occur and share overlapping symptoms, creating challenges for accurate and timely diagnosis. Research suggests that approximately 50% of individuals live with an undiagnosed mental health condition and at least 65% of conditions may be misdiagnosed. Diagnosis typically begins with a clinical interview followed by one or more screening tools based on initial impressions. However, selecting individual assessments may cause comorbidities to be overlooked, and arriving at a diagnosis does not guarantee its accuracy.
MindMetrix was developed to address this challenge through a comprehensive assessment that dynamically administers validated self-report scales in a staged digital questionnaire, ultimately screening for more than 60 different mental health conditions. This study evaluated how MindMetrix impacts patient outcomes on self-reported depression, anxiety, and ADHD symptom severity over time.
How MindMetrix Works
The poster included a visual overview of the MindMetrix assessment process, illustrating its three-stage approach.
1. Initial Symptom Screen
Patients indicate whether key symptoms associated with a broad range of psychiatric disorders describe problems or experiences they have had currently or at some point in their lives. Follow-up questions assess the daily impact of those symptoms.
Symptoms and impact items that meet predetermined gating thresholds trigger additional disorder-specific follow-up testing.
2. Disorder-Specific Follow-Up Test Sets
Each follow-up test set contains up to three validated self-report assessments tailored to the symptom profile identified during the initial screening stage.
3. Probability Estimates for Each Disorder
MindMetrix estimates disorder probabilities by applying Bayes' theorem to published sensitivity and specificity values and weighting those results by disorder prevalence to create likelihood ratios.
Methods
Study Design
Researchers conducted a single-site, retrospective longitudinal analysis of electronic medical records from a regional outpatient psychiatric center. Adult patients who received treatment between October 2023 and June 2024 were eligible for inclusion. Patients were required to have:
- A Clinical Global Impression-Severity (CGI-S) score of 4 or greater at their first visit
- At least one recorded visit with a prescriber
Patient Groups
MindMetrix was incorporated into intake procedures through a clinical rollout process.
Researchers compared:
- Patients who completed MindMetrix during intake (+MM, n = 97)
- Patients who completed standard intake procedures without MindMetrix (-MM, n = 50)
The comparison group was selected to be as similar as possible to the MindMetrix group. Baseline comparability was confirmed using independent samples t-tests across all primary outcome measures, with no significant differences observed at baseline.
Assessments
All patients completed a digital pre-visit survey before intake and before subsequent appointments. The survey included:
- PHQ-9 for depression
- GAD-2 for anxiety
- ASSET for ADHD symptom severity
Clinicians also recorded a CGI-S score at each visit.
Statistical Analysis
Researchers calculated change from baseline (CFB) scores for PHQ-9, GAD-2, and ASSET at the first follow-up visit occurring between 90 and 120 days after intake.
Additional analyses included:
- Pearson correlations
- Principal axis factoring to derive a composite psychiatric symptom burden score
- Linear regression models examining whether MindMetrix moderated the relationship between time in treatment and symptom improvement
Study Population
The study included 147 patients. Mean age was 35.82 years (SD = 13.09), and 67.1% were female. The sample was predominantly White (86.3%), with smaller proportions identifying as Black (6.85%), Hispanic (4.11%), or another race (1.4%).
Results
Baseline Comparability
Baseline CGI-S, PHQ-9, GAD-2, and ASSET scores did not differ significantly between the MindMetrix and non-MindMetrix groups, supporting comparability before treatment outcomes were examined.
Retention and Attrition
Sixty-four percent of patients had a follow-up visit between 90 and 120 days after intake.
Patients who completed MindMetrix were significantly more likely to remain in treatment at 90 days than patients who completed standard intake procedures:
- MindMetrix: 70.8%
- No MindMetrix: 46.9%
- Odds Ratio = 2.75
- p = .006
Among patients with elevated baseline ADHD symptom burden (ASSET ≥ 4.40), the difference was even larger:
- MindMetrix: 72.7% retained
- No MindMetrix: 26.7% retained
- Odds Ratio = 7.33
- p = .002
Symptom Improvement
The poster included trajectory plots displaying longitudinal symptom change over as many as 300 days of follow-up. The visualizations compared patients who completed MindMetrix with those who did not across three outcomes:
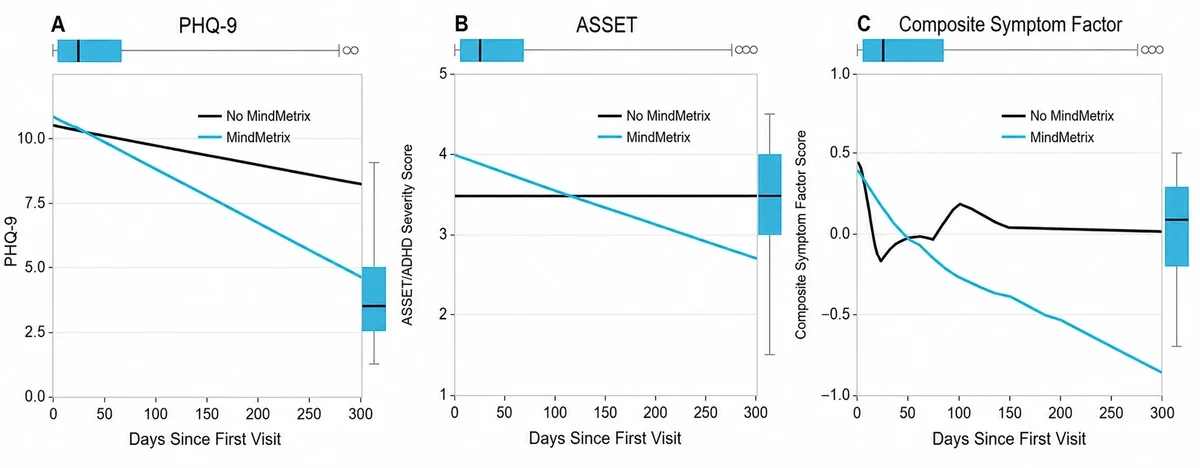
Figure 1A: PHQ-9 depressive symptom severity
Figure 1B: ASSET ADHD symptom severity
Figure 1C: Composite psychiatric symptom burden score derived from PHQ-9, GAD-2, and ASSET scores
In each figure, LOESS-smoothed trend lines illustrated symptom trajectories over time. Patients who completed MindMetrix demonstrated steeper declines in depressive symptoms, ADHD symptoms, and overall psychiatric symptom burden. Box plots along the horizontal and vertical axes displayed distributions of follow-up duration and symptom scores.
Associations with MindMetrix and Time in Treatment
MindMetrix completion and days in treatment were each independently associated with greater improvement in:
- PHQ-9 depression scores
- GAD-2 anxiety scores
- ASSET ADHD scores
All associations were statistically significant.
Moderation Effects
Regression analyses found that MindMetrix significantly moderated the relationship between time in treatment and:
Depression (PHQ-9)
β = -0.857, p = .049
Patients who completed MindMetrix experienced steeper improvement trajectories over time.
ADHD Symptoms (ASSET)
β = -0.307, p = .002
Patients who completed MindMetrix again demonstrated steeper symptom improvement trajectories.
Anxiety (GAD-2)
β = -0.184, p = .158
No statistically significant moderation effect was observed for anxiety symptoms.
Overall Psychiatric Symptom Burden
The strongest moderation effect was observed for the composite psychiatric symptom factor score:
β = -0.256, p = .001
Conclusions and Limitations
This study was the first to empirically suggest that including MindMetrix, a comprehensive dynamically administered mental health assessment, in the intake protocol for patients referred for mental health treatment is associated with improved symptom trajectories.
Researchers found that:
- Depression, ADHD, and composite mental health symptoms improved as patients spent more time in treatment regardless of MindMetrix completion.
- MindMetrix designation was associated with steeper symptom improvement trajectories over time for depression and ADHD, but not anxiety.
- MindMetrix exhibited the strongest effect on overall psychiatric symptom burden.
The authors also noted several limitations. As with all real-world evidence studies, conclusions are descriptive, residual confounding remains possible, and generalizability is not guaranteed. They recommend future research replicating these findings in more diverse populations and through experimental study designs.
Funding
This study was funded by MindMetrix, LLC.
Present at NEI Spring Congress
Evaluating the impact of MindMetrix, a dynamic and comprehensive mental health assessment, on psychiatric symptoms over time was presented at the NEI Spring Congress, May 1–3, 2026, by researchers from Rochester Center for Behavioral Medicine, MedaData, Wayne State University, Oakland University, and MindMetrix.
Ready to boost your practice?
Try 3 complimentary assessments on us.