Offsetting the Cost of MindMetrix

Strategies That Work
July, 2026
One of the most common questions we hear from clinicians considering MindMetrix is: "How do practices recover the cost of using MindMetrix?"
MindMetrix itself isn't the billable service. The assessment is completed independently by the patient, often before or between appointments.
What is billable is the clinical work you already perform: reviewing the results, integrating them into your diagnostic formulation, discussing findings with the patient, and incorporating them into your treatment plan.
Every practice has a slightly different workflow, payer mix, and documentation process, so there isn't one universal approach. Below are five billing strategies we've seen practices successfully implement. Your billing team can help determine which option best fits your organization.
This resource is for educational purposes only and should not be considered legal, coding, or billing advice. Coverage and reimbursement vary by payer, provider credential, contract, and state law. Always verify coding requirements with your billing team, certified coder, or insurance payer before submitting claims.
Option 1: Bill CPT 96130 During the Next Scheduled Visit (Most Common)
For many practices, this is the simplest and most efficient workflow because it doesn't require adding another appointment to the schedule.

Practices commonly bill:
- 99213-99215 for the office visit
- Modifier 25 on the E/M service
- 96130 with Modifier 59 to indicate a distinct service
- Modifier 95 when performed via telehealth, if applicable
Remember that 96130 requires at least 31 minutes of total evaluation and interpretation time, which may include:
- Reviewing the assessment results before the visit
- Interpreting findings
- Discussing results with the patient
- Integrating the information into diagnosis and treatment planning
- Documenting your clinical conclusions
For many practices, this workflow fits naturally into existing follow-up appointments without creating additional scheduling burden.
Option 2: Review Results During the Initial Evaluation
Some practices prefer to have patients complete MindMetrix before their very first appointment.
This allows clinicians to begin the diagnostic interview with structured clinical data already available, helping focus the conversation and potentially improving diagnostic efficiency.

In this workflow, the MindMetrix review is incorporated into the initial psychiatric evaluation rather than waiting until a second visit.
Before using this approach, confirm with your billing team whether your payers allow 96130 and 90791/90792 on the same date of service. Some payers require these services to occur on separate days.
Option 3: Schedule a Dedicated Results Review Visit
If reimbursement for 96130 has been inconsistent with certain payers, some practices choose to schedule a brief, dedicated appointment focused on reviewing the assessment results.
During this visit, clinicians often bill:
- 99213-99215 (based on medical decision-making or time)
- 90833 when appropriate therapeutic discussion occurs during the same visit

This option works well for practices that already conduct formal feedback sessions or want dedicated time to discuss diagnostic impressions and treatment recommendations.
Because this represents an additional clinical encounter, it should only be used when it fits your scheduling model.
Option 4: Charge a Patient Assessment Fee
This option applies only to practices using MindMetrix's provider subscription model, not patient-pay pricing.
If insurance reimbursement is not appropriate for your workflow, some practices elect to charge patients directly for the digital assessment experience.
Before implementing a patient-pay assessment fee, review:
- Payer participation agreements
- State regulations
- Internal compliance policies
Many practices appreciate having this flexibility when working with payer mixes that do not consistently reimburse testing evaluation services.
Option 5: Use Standalone Rating Scale Codes
Some insurance plans do not reimburse 96130 consistently.
In these situations, practices may instead bill standardized assessment codes such as 96127 for the individual rating scales included within the assessment.
While reimbursement is generally lower (often around $5–15 per unit, depending on payer), 96127 is widely accepted, including by Medicare.
Keep in mind that many payers limit reimbursement to three or four units per visit, and 96127 generally should not be billed on the same day as 96130, 96136, or 96138.
For some practices, this provides a useful alternative when testing evaluation services are not covered.
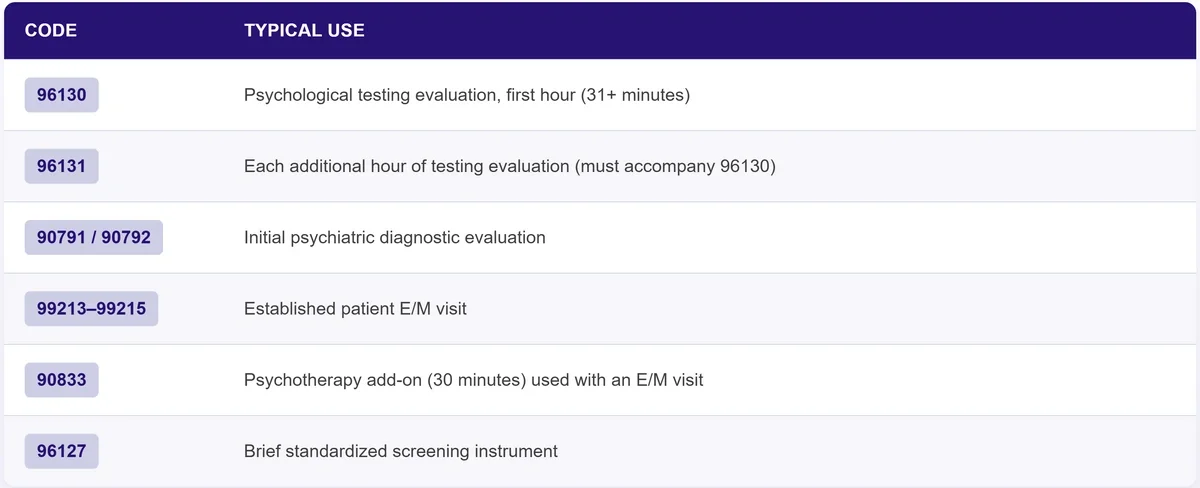
Quick Reference: Common Codes
Questions About Your Billing Workflow?
Our team is happy to share what we've seen work across practices and connect you with additional billing resources.
Need help? Schedule a billing consultation with our team.
For more detailed coding guidance, documentation tips, and code definitions, read our Complete CPT 96130 Billing Guide.
Ready to boost your practice?
Try 3 complimentary assessments on us.